Do Cholesterol Medications Defeat Exercise Programs?
What You Should Know Before You Take a Statin
Statins are among the most widely prescribed drugs in the world. They lower LDL cholesterol and reduce the risk of heart attack and stroke, and for millions of people they are genuinely lifesaving. But like any powerful medication, they come with trade-offs that don't always get discussed in the ten minutes you spend with your doctor. If you're taking a statin or considering one, here's what the current evidence actually shows.
They work. But not for everyone equally.
The strongest case for statins is in people who already have cardiovascular disease or who have had a heart attack or stroke. For those patients, the evidence that statins reduce the risk of future events and death is clear and consistent across multiple large randomized trials. This is called secondary prevention, meaning the drug is preventing a second event in someone already known to have heart disease.
For people who have never had a cardiovascular event, the picture is more nuanced. This is called primary prevention, and the benefit is real but smaller in absolute terms.
The American College of Cardiology (ACC) and American Heart Association (AHA) guidelines recommend considering statins for primary prevention in adults aged 40 to 75 with at least one cardiovascular risk factor and a calculated ten-year risk of 7.5% or higher.
The U.S. Preventive Services Task Force sets a stronger threshold, giving its clearest recommendation at a ten-year risk of 10% or above. Across that range, meta-analyses typically find about a 20 to 25% relative reduction in major cardiovascular events for every significant drop in LDL.
One important caveat: the evidence for primary prevention is strongest up to around age 75. Beyond that, the data becomes less consistent and the decision requires a careful individual conversation with your doctor.
They can affect your blood sugar.
This is real and worth knowing about. Some studies have found up to a 46% higher relative risk of developing type 2 diabetes among statin users, but that figure comes from one large Finnish observational study and is higher than what most randomized trials report. Pooled analyses of clinical trials generally find a smaller increase, typically around 9 to 12%, with higher risks seen in people taking high-dose statins or those already predisposed to diabetes.
Across multiple trials, the absolute impact works out to roughly one to two extra diabetes cases per 100 higher-risk people treated over several years, and likely fewer than that in lower-risk populations. The FDA added a diabetes warning to statin labels in 2012, though the agency continues to conclude that for most patients the cardiovascular benefits outweigh the risks.
The people most likely to be affected are those who already had elevated diabetes risk before starting a statin: people with prediabetes, obesity, metabolic syndrome, or a strong family history of diabetes. The statin usually isn't creating a new problem from scratch. It's nudging an existing vulnerability a little further along.
Several mechanisms have been proposed for why this happens. One hypothesis involves a compound called GGPP, which statins reduce as a downstream effect of blocking cholesterol production. Laboratory studies suggest GGPP plays a role in helping muscle cells absorb glucose and in the pancreas releasing insulin properly. But human research points to multiple overlapping pathways rather than one single cause. If your blood sugar or A1c starts drifting upward after starting a statin, that's worth raising with your doctor. It's not a reason to stop the medication on your own.
To put the trade-off in perspective: for a person at moderate to high cardiovascular risk, statins typically prevent several heart attacks and strokes for every additional diabetes case they may contribute to. The math generally favors the statin for high-risk patients, while becoming a closer call for lower-risk individuals.
They may affect your exercise gains, but probably less than one famous study suggested.
A 2013 study from Duke University found that people taking simvastatin while following a twelve-week exercise program had substantially blunted fitness gains compared to people exercising without the drug. The statin group's aerobic capacity and muscle adaptation were significantly worse. That finding got a lot of attention.
What happened next got less attention. Subsequent research has not consistently confirmed that dramatic effect. A review of multiple studies found limited evidence that statins impair exercise capacity for most people, and concluded that the benefits of staying active while on a statin clearly outweigh the risks. Of ten studies that examined statin effects on aerobic performance, only three found that statins reduced it.
Exercise still works. It still improves cardiovascular fitness and metabolic health in people on statins. High-dose statins, particularly simvastatin, may blunt some of the adaptation your muscles make in response to training, particularly around mitochondrial function. But that's different from saying exercise stops working.
The muscle pain question.
Muscle aches are the most commonly reported side effect of statins, and they're one of the main reasons people stop taking the medication. The full picture here is more complicated than it first appears. In real-world clinical practice, somewhere between 5 and 20% of statin users report muscle symptoms. But when researchers run blinded placebo-controlled trials, where neither patients nor doctors know who is taking the drug, the rates of muscle complaints are nearly identical in the statin and placebo groups.
That tells us a meaningful portion of reported muscle pain may be what researchers call the nocebo effect, meaning the expectation of side effects can produce them. Even so, a genuine subset of patients does develop real statin-related muscle problems, and in rare cases a serious condition called rhabdomyolysis, involving significant muscle breakdown, can occur. If your muscle pain is severe, persistent, or accompanied by dark urine, that's a medical conversation you need to have right away.
The connection to CoQ10, which statins also reduce via the same cholesterol-making pathway, is biologically plausible. But meta-analyses and guideline bodies have generally concluded there isn't enough evidence to recommend CoQ10 routinely for statin-related muscle symptoms, though some patients report subjective benefit.
What this means for you.
If your cholesterol numbers improved after starting a statin, the medication is likely contributing to that, though lifestyle changes often play an important role too. If your blood sugar is creeping up, your muscles ache regularly, or you feel like your workouts aren't producing results, those are legitimate concerns worth raising with your doctor. Don't stop your statin on your own. For high-risk patients especially, stopping suddenly can significantly increase the risk of heart attack or stroke. Changes should be made thoughtfully, and usually with a doctor involved.
That conversation might include adjusting your dose, switching to a different statin, since not all statins carry equal risks for these side effects, or exploring other cholesterol-lowering options if statins aren't working for you.
Statins are powerful medications with real benefits and real trade-offs. The goal isn't to fear them or to take them without thinking. It's to understand them well enough to make decisions with your doctor based on your actual risk, your actual numbers, and your actual life.
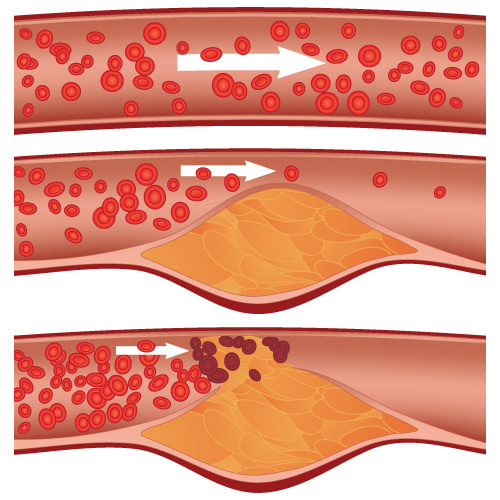
The top artery is healthy. The middle and bottom arteries show plaque formation, rupturing, clotting and blood flow interruption.
To learn more about cholesterol, click here.
Reference Links:
Statin Use for the Primary Prevention of Cardiovascular Disease in Adults
US Preventive Services Task Force Recommendation Statement
JAMA Network, Published Online: August 23/30, 2022
Click Here for the Statement: https://doi.org/10.1001/jama.2022.13044
2026 ACC/AHA/AACVPR/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Dyslipidemia: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines
Roger S. Blumenthal, Pamela B. Morris, Mario Gaudino, Heather M. Johnson, Timothy S. Anderson, Vera A. Bittner, Ron Blankstein, LaPrincess C. Brewer, Leslie Cho, Sarah D. de Ferranti, Eugenia Gianos, Ty J. Gluckman, Kristen F. Gradney, Ijeoma Isiadinso, Donald M. Lloyd-Jones, Joel C. Marrs, Seth S. Martin, Kellie H. McLain, Laxmi S. Mehta, Samia Mora, Wudeneh M. Mulugeta, Pradeep Natarajan, Ann Marie Navar, Carl E. Orringer, Tamar S. Polonsky, Harmony R. Reynolds, Joseph J. Saseen, Michael D. Shapiro, Daniel E. Soffer, Sheila A. Tynes, Chloé D. Villavaso, Salim S. Virani, and John T. Wilkins
JACC JOURNALS, Published 13 March 2026
Click Here for the Guidelines: https://www.jacc.org/doi/10.1016/j.jacc.2018.11.002
Primary prevention statin therapy in older adults
Nanna, Michael G.; Abdullah, Ahmeda; Mortensen, Martin B.; Navar, Ann Marie
Current Opinion in Cardiology, Published 38(1):p 11-20, January 2023.
Click Here for the Study: https://doi.org/10.1097/HCO.0000000000001003
Increased risk of diabetes with statin treatment is associated with impaired insulin sensitivity and insulin secretion: a 6 year follow-up study of the METSIM cohort
Henna Cederberg, Alena Stančáková, Nagendra Yaluri, Shalem Modi, Johanna Kuusisto & Markku Laakso
Diabetologia, Published 10 March 2015
Click Here for the Study: https://link.springer.com/article/10.1007/s00125-015-3528-5
Statins and risk of incident diabetes: a collaborative meta-analysis of randomised statin trials
Prof Naveed Sattar, PhDa Send email to nsattar@clinmed.gla.ac.uk ∙ Dr David Preiss, MRCPa Send email to d.preiss@clinmed.gla.ac.uk ∙ Heather M Murray, MScb ∙ Paul Welsh, PhDa ∙ Prof Brendan M Buckley, FRCPIc ∙ Anton JM de Craen, PhDd ∙ Sreenivasa Rao Kondapally Seshasai, MDe ∙ Prof John J McMurray, MDa ∙ Dilys J Freeman, PhDf ∙ Prof J Wouter Jukema, MDg ∙ Prof Peter W Macfarlane, DSch ∙ Prof Chris J Packard, DSch ∙ Prof David J Stott, MDh ∙ Prof Rudi G Westendorp, MDi ∙ Prof James Shepherd, MDh ∙ Prof Barry R Davis, PhDj ∙ Sara L Pressel, MSj ∙ Prof Roberto Marchioli, MDk ∙ Prof Rosa Maria Marfisi, MSk ∙ Prof Aldo P Maggioni, MDl ∙ Prof Luigi Tavazzi, MDm ∙ Prof Gianni Tognoni, MDk ∙ Prof John Kjekshus, MDn ∙ Prof Terje R Pedersen, MDo ∙ Thomas J Cook, MSp ∙ Prof Antonio M Gotto, MDq ∙ Prof Michael B Clearfield, DOr ∙ John R Downs, MDs ∙ Prof Haruo Nakamura, MDt ∙ Prof Yasuo Ohashi, MDu ∙ Prof Kyoichi Mizuno, MDv ∙ Kausik K Ray, MDe ∙ Prof Ian Ford, PhD
THE LANCET, Published February 27, 2010
Click Here for the Study: https://www.thelancet.com/journals/lancet/article/PIIS0140673609619656/fulltext
Geranylgeranyl pyrophosphate depletion by statins compromises skeletal muscle insulin sensitivity
Lai Wang, Zuguo Zheng, Lijun Zhu, Lingchang Meng, Hanling Liu, Keke Wang, Jun Chen, Ping Li, Hua Yang
Journal of Cachexia, Sarcopenia and Muscle, Published 12 August 2022
Click Here for the Study: https://doi.org/10.1002/jcsm.13061
Simvastatin Impairs Exercise Training Adaptations
Catherine R. Mikus, PhD, Leryn J. Boyle, MSc, Sarah J. Borengasser, PhD, Douglas J. Oberlin, MSc, Scott P. Naples, MSc, Justin Fletcher, MSc, Grace M. Meers, BSc, Meghan Ruebel, MA, M. Harold Laughlin, PhD, Kevin C. Dellsperger, MD, PhD, Paul J. Fadel, PhD, and John P. Thyfault, PhD
JACC Journals
, Published 10 April 2013
Click Here for the Study: https://www.jacc.org/doi/abs/10.1016/j.jacc.2013.02.074
The impact of statins on physical activity and exercise capacity: an overview of the evidence, mechanisms, and recommendations
Allyson M. Schweitzer, Molly A. Gingrich, Thomas J. Hawke & Irena A. Rebalka
European Journal of Applied Physiology, Published 04 April 2020
Click Here for the Study: https://link.springer.com/article/10.1007/s00421-020-04360-2
Statins and risk of type 2 diabetes: mechanism and clinical implications
Markku Laakso & Lilian Fernandes Silva
Frontiers in Endocrinology, Published 18 September 2023
Click Here for the Study: https://www.frontiersin.org/journals/endocrinology/articles/10.3389/fendo.2023.1239335/full
Call for a FREE Consultation (305) 296-3434
CAUTION: Check with your doctor before
beginning any diet or exercise program.
7/7/2013
Updated 9/29/2020
Updated 4/23/2026
Updated 6/23/2026


