Cholesterol and Your Health
How Low Should Your Cholesterol Go?
There are many misconceptions about cholesterol: what it does to our bodies, how medications work, and what a “healthy” number really is. Let’s clear up some of that confusion.
What is cholesterol?
The American Heart Association explains it this way:
“Cholesterol is a waxy substance. It’s not inherently ‘bad.’ Your body needs it to build cells and make vitamins and other hormones. But too much cholesterol can pose a problem.”
Your liver makes all the cholesterol you need. The rest comes from foods from animals, like meat, poultry, and dairy products. Those foods also tend to be high in saturated and sometimes trans fats. Those fats can push your liver to make more cholesterol than it otherwise would. In some people, that is enough to move them from a normal cholesterol level into an unhealthy range.
Are there different types of cholesterol?
Two main lipoproteins carry cholesterol in your blood:
LDL (low density lipoprotein) is often called “bad” or "lousy" cholesterol. Higher LDL is strongly linked to plaque buildup in arteries and a higher risk of heart disease and stroke.
HDL (high density lipoprotein) is often called “good” or "healthy" cholesterol. Higher HDL is generally associated with lower cardiovascular risk, although simply raising HDL with drugs has not reliably reduced events.
HDL is the HEALTHY or GOOD cholesterol. LDL is the LOUSY or BAD cholesterol.
What do the cholesterol numbers mean?
Let’s focus on LDL, because that is the main treatment target in most guidelines.
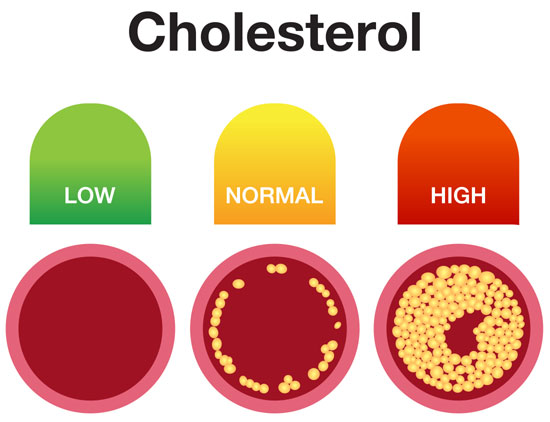
When your body has too much LDL cholesterol, it can deposit in the walls of your blood vessels. Over years, those deposits form plaque. The more plaque, the narrower and stiffer your arteries become, and the easier it is for a clot or rupture to trigger a heart attack or stroke.
Typical reference ranges look like this:
Children and teens (up to about 19): LDL below 110 mg/dL is generally considered acceptable.
Adults (20 and older):
For people at lower cardiovascular risk, many expert groups consider LDL below 100 mg/dL a reasonable goal.
For people at higher risk, because of existing heart disease, diabetes, kidney disease, or a very high calculated 10 year risk, more recent recommendations often aim for below about 70 mg/dL, and sometimes lower for those at very high risk.
Those are not hard and fast rules for everyone. They are targets your doctor uses in the context of your overall risk profile.
Why is controlling LDL cholesterol essential?
Heart disease remains the leading cause of death for men and women in the United States. The most common underlying problem is atherosclerosis: plaque buildup and narrowing in the coronary arteries that supply blood to your heart.
Classic autopsy studies of thousands of young people who died from accidents, homicides, or suicides found that many teenagers already had fatty streaks in their arteries.
A substantial percentage of people in their 20s and early 30s had more advanced plaques.
In other words, atherosclerosis often begins in youth, long before symptoms. If you wait to deal with high LDL until problems show up, you are treating after years of silent damage, and it is harder to fully change your trajectory.
Why don't cholesterol lowering drugs “fix” everything?
A common frustration goes like this: “My LDL went down on the medication, but I still have plaque. Why didn’t the drug clean it all up?”
The reason is cumulative exposure. If your LDL has been elevated for years or decades, your arteries have already seen a lot of cholesterol. Starting a statin or other LDL lowering drug at that point is still very beneficial. It lowers LDL, helps stabilize plaque, and reduces your risk of heart attack and stroke. But it cannot instantly erase decades of buildup.
Think of it this way. Drugs mainly change the slope of the curve going forward. They can stabilize existing plaques and sometimes produce modest regression, but the earlier in life you lower LDL, and the longer you keep it low, the bigger the lifetime payoff.
That is why early prevention and long term control matter, not just what your LDL is this year.

How low should your cholesterol go?
Most lab reports show a single “normal” range for LDL, but your personal target should depend on two things.
1. Your current and future risk, for example whether you have heart disease, diabetes, or a strong family history.
2. How much high LDL your arteries have already seen over your lifetime.
A helpful way to think about it:
1. Lifetime exposure matters as much as the current number.
Genetic and long term observational studies show that people who have modestly lower LDL from early in life have dramatically fewer heart attacks than people who spend decades at higher levels. A small difference in LDL, multiplied over decades, adds up to a big difference in cumulative damage.
By contrast, when we start medication later in life, drug trials still show meaningful risk reductions, but the benefit is smaller because we are intervening after many years of exposure.
2. Higher past LDL means a lower target needed now.
Because of that, your past history shifts how low you may need to go now:
If you have spent most of your life with LDL in a near optimal range and you do not have other major risk factors, your doctor might be comfortable with a goal around what many experts consider “optimal,” roughly 50 to 70 mg/dL, or even a bit higher in truly low risk people.
If you have had years or decades of clearly elevated LDL, for example often in the 130s, 150s, or higher, or you have multiple risk factors like smoking, hypertension, or a strong family history, your arteries have already seen much more LDL. To significantly slow or stop plaque progression, your care team may aim for below about 70 mg/dL, and sometimes into the 50 to 60 mg/dL range.
If you are in a very high risk group, such as having already had a heart attack, having multiple blocked vessels, or having conditions like familial hypercholesterolemia, your cardiologist may target even lower LDL levels, often in the 30 to 50 mg/dL range, because clinical trials show that pushing LDL that low in these patients can further reduce events and appears safe over the lengths of follow up we have.
There is not a single “magic number” that applies to everyone. Instead, the higher your lifetime LDL exposure and the higher your risk, the lower your LDL target usually needs to be today to meaningfully change your future risk.
3. Where lifestyle fits in.
Large cohort studies also show that people who keep up multiple healthy lifestyle habits, do not smoke, stay active, eat a heart healthy diet, maintain a healthy weight, have dramatically fewer heart attacks than people with very unhealthy lifestyles. In some analyses, ideal lifestyle patterns are associated with roughly 80 to 90 percent lower risk of a first heart attack compared with very poor patterns.
That does not mean lifestyle replaces medication for everyone. Lifestyle started early can keep LDL and other risk factors low enough that you may never need aggressive drug therapy.
If you are already high risk, lifestyle plus medication together give you the best shot at lowering risk, and lifestyle helps you get the most out of whatever LDL lowering target you and your doctor decide on.
What should I do?
You cannot go back and change what your LDL was when you were younger, but you can change what happens from today forward.
Eat for your arteries. Emphasize vegetables, fruits, whole grains, beans, nuts, seeds, and plant based oils. Reduce saturated fat from fatty meats, full fat dairy, butter, and tropical oils, and keep added sugars and highly processed foods in check.
Move more, sit less. Regular cardio and resistance training help improve your lipid profile, blood pressure, insulin sensitivity, and overall cardiovascular health.
Know your risk. If your LDL is high or you have other risk factors, talk with your doctor about your overall cardiovascular risk and what LDL range makes sense for you. For some people, especially those with established heart disease, familial hypercholesterolemia, or very high risk, medication is not optional, it is a cornerstone of staying alive and well. For others at lower risk, intensive lifestyle changes may carry more of the load, with medication as a tool if needed.
The bottom line:
High LDL is not a single number with a single fix. The higher and longer your LDL has been elevated, the lower you will usually need to bring it, often below what a lab calls “ideal,” to meaningfully change your risk. The best approach is almost always a combination of lifestyle and, when indicated, medication, tailored to your actual history and your actual risk.
Reference Links:
Determinants of atherosclerosis in the young. Pathobiological Determinants of Atherosclerosis in Youth (PDAY) Research Group
H C McGill Jr, C A McMahan
The American Journal of Cardiology, 1998 Nov 26;82(10B):30T-36T. doi: 10.1016/s0002-9149(98)00720-6.
Click Here for the study: https://pubmed.ncbi.nlm.nih.gov/9860371/
Prevalence and extent of atherosclerosis in adolescents and young adults: implications for prevention from the Pathobiological Determinants of Atherosclerosis in Youth Study
J P Strong, G T Malcom, C A McMahan, R E Tracy, W P Newman 3rd, E E Herderick, J F Cornhill
JAMA, 1999 Feb 24;281(8):727-35. doi: 10.1001/jama.281.8.727.
Click Here for the study: https://pubmed.ncbi.nlm.nih.gov/10052443/
Sequence variations in PCSK9, low LDL, and protection against coronary heart disease
Jonathan C Cohen, Eric Boerwinkle, Thomas H Mosley Jr, Helen H Hobbs
The New England Journal of Medicine, 2006 Mar 23;354(12):1264-72. doi: 10.1056/NEJMoa054013.
Click Here for the Study: https://pubmed.ncbi.nlm.nih.gov/16554528/
Optimal low-density lipoprotein is 50 to 70 mg/dl: lower is better and physiologically normal
James H O'Keefe Jr, Loren Cordain, William H Harris, Richard M Moe, Robert Vogel
Journal of the American College of Cardiology, 2004 Jun 2;43(11):2142-6. doi: 10.1016/j.jacc.2004.03.046.
Click Here for the study: https://pubmed.ncbi.nlm.nih.gov/15172426/
Evidence Mandating Earlier and More Aggressive Treatment of Hypercholesterolemia
Daniel Steinberg, Christopher K. Glass, and Joseph L. Witztum
American Heart Association - Circulation, 5 Aug 2008 https://doi.org/10.1161/CIRCULATIONAHA.107.753152Circulation. 2008;118:672–677
Click Here for the study: https://www.ahajournals.org/doi/10.1161/CIRCULATIONAHA.107.753152
Position of the Academy of Nutrition and Dietetics: Vegetarian Diets
Vesanto Melina, Winston Craig, Susan Levin
Journal of the Academy of Nutrition and Dietetics, 2016 Dec;116(12):1970-1980. doi: 10.1016/j.jand.2016.09.025.
Click Here for the study: https://pubmed.ncbi.nlm.nih.gov/27886704/
Can low-density lipoprotein be too low? The safety and efficacy of achieving very low low-density lipoprotein with intensive statin therapy: a PROVE IT-TIMI 22 substudy
Stephen D Wiviott, Christopher P Cannon, David A Morrow, Kausik K Ray, Marc A Pfeffer, Eugene Braunwald, PROVE IT-TIMI 22 Investigators
Journal of the American College of Cardiology, 2005 Oct 18;46(8):1411-6. doi: 10.1016/j.jacc.2005.04.064.
Click Here for the study: https://pubmed.ncbi.nlm.nih.gov/16226163/
Call for a FREE Consultation (305) 296-3434
CAUTION: Check with your doctor before
beginning any diet or exercise program.
12/20/2021
Updated 6/23/2026


